About SBIRT
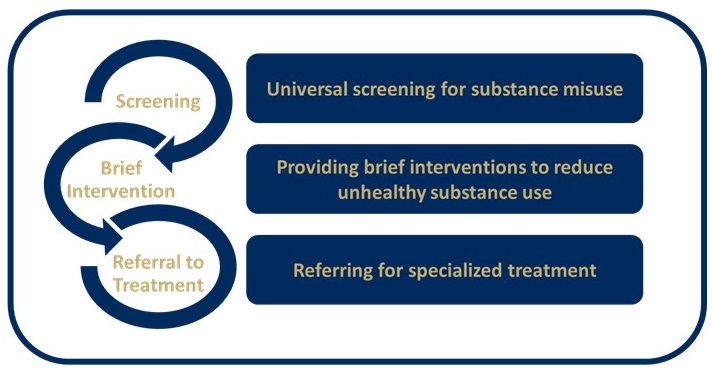
What is SBIRT?
SBIRT is a comprehensive and integrated public health approach to the delivery of early intervention and treatment services through universal screening for persons with substance use disorders (SUD) and those at risk of developing these disorders.
Babor, T. F., Del Boca, F., & Bray, J. W. (2017). Screening, Brief Intervention and Referral to Treatment: implications of SAMHSA's SBIRT initiative for substance abuse policy and practice. Addiction, 112 Suppl 2, 110-117. doi:10.1111/add.13675
Why practice SBIRT?
Substance use disorders (SUDs) and harmful drug and alcohol use are increasing problems in the United States.
The 2017 National Survey on Drug Use and Health estimated that:
- 66.6 million individuals (24.5% of the U.S. population, aged 12 and older) are misusing alcohol.
- 30.5 million individuals (11.2% of the U.S. population, aged 12 and older) are misusing drugs.
- 19.7 million individuals (7.2% of the population) meet criteria for a DSM-IV SUD.
Misuse of alcohol and other drugs is significantly associated with medication adherence problems, overdose deaths, trauma and injury, and poor health outcomes (i.e., stroke, heart attacks, diabetes, etc.). A significant proportion of patients who misuse alcohol or drugs are likely to be present in different healthcare settings. It is estimated that:
- 23.4% of primary care patients in the U.S., aged 18 and older, are misusing alcohol or drugs.
- 39.9% of emergency department patients in the U.S., aged 18 and older, are misusing alcohol or drugs.
Substance misuse and SUDs are associated directly with increased healthcare and other social costs. The estimated total annual cost associated with substance misuse and SUD in United States is more than $740 billion, including costs associated with crime, lost work productivity, and health care. Despite this enormous cost, only 10% of patients with SUDs receive treatment.
SBIRT is one method for identifying and intervening with individuals earlier in their risk trajectory. Research has demonstrated SBIRT’s many benefits, including reductions in healthcare costs, severity of substance use, and trauma1-3. In addition to these reductions, SBIRT application in healthcare sites can help healthcare systems achieve optimal performance with the Healthcare Effectiveness Data and Information Set (HEDIS) measure regarding initiation and engagement of appropriate patients in alcohol or drug (AOD) treatment. SBIRT’s demonstrated cost savings and health impacts have led federal agencies such as Substance Abuse and Mental Health Services (SAMHSA), Veterans Administration, Department of Defense, and the White House Office of National Drug Control Policy to recommend routine SBIRT use. The United States Preventative Services Task Force recommends SBIRT for alcohol misuse in adults (18+ years) and gave it a “B” rating, which is the same rating assigned to screening for obesity, diabetes, and breast cancer.
Please see the resources below for evidence on the cost-effectiveness of SBIRT implementation:
- Screening, Brief Intervention, and Referral to Treatment in the Emergency Department from the journal Medical care.
- Missouri Screening, Brief Intervention, Referral and Treatment: An Analysis of National Funding Trends for SBI Services from Missouri Institute of Mental Health
- A Cost-Benefit Analysis of Wisconsin’s Screening, Brief Intervention, and Referral to Treatment Program: Adding the Employer’s Perspective from Quanbeck, Lang, Enami, and Brown of the University of Wisconsin
- Alcohol Cost Calculator from The George Washington University Medical Center
How is SBIRT different from past approaches to SUD treatment?
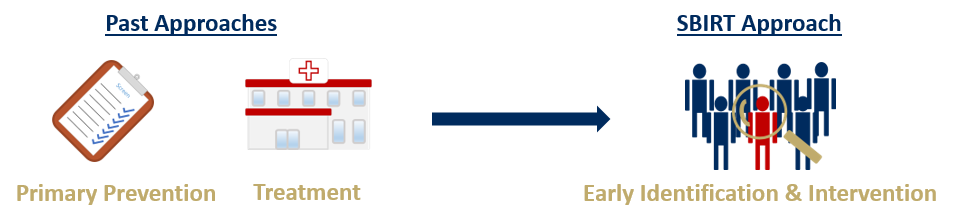
A paradigm shift has occurred with regards to SUD treatment as past approaches have typically focused on SUDs through primary prevention or treatment of individuals with severe SUD, while SBIRT focuses on early intervention and the identification of individuals at an early stage of substance misuse, prior to the development of an SUD.
(1) Barbosa, C., Cowell, A., Bray, J., & Aldridge, A. (2015). The cost-effectiveness of alcohol screening, brief intervention, and referral to treatment (SBIRT) in emergency and outpatient medical settings. J Subst Abuse Treat, 53, 1-8. doi:10.1016/j.jsat.2015.01.003 (2) Bray, J. W., Del Boca, F. K., McRee, B. G., Hayashi, S. W., & Babor, T. F. (2017). Screening, Brief Intervention and Referral to Treatment (SBIRT): rationale, program overview and cross-site evaluation. Addiction, 112 Suppl 2, 3-11. doi:10.1111/add.13676 (3) Babor, T. F., Del Boca, F., & Bray, J. W. (2017). Screening, Brief Intervention and Referral to Treatment: implications of SAMHSA's SBIRT initiative for substance abuse policy and practice. Addiction, 112 Suppl 2, 110-117. doi:10.1111/add.13675
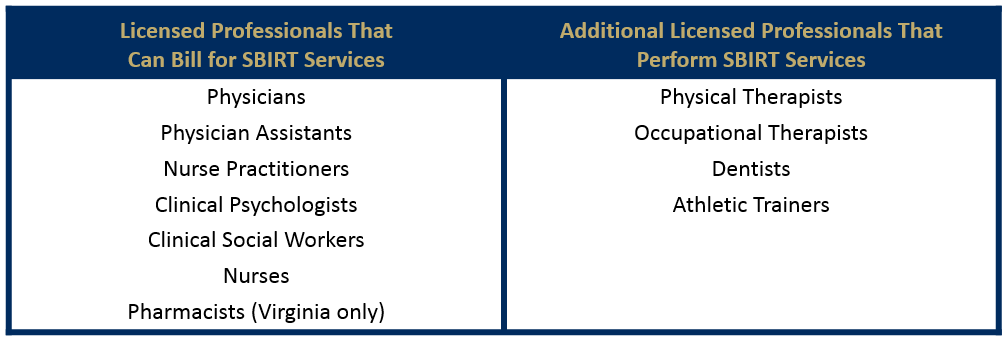
Who practices SBIRT?
Many commercial insurers reimburse for SBIRT services. However, a variety of licensed health professionals perform SBIRT services.
Where is SBIRT practiced?
The SBIRT practice can be utilized in a variety of healthcare settings, such as:
- Primary Care;
- Emergency Departments;
- Hospitals;
- Pharmacies;
- Physical Rehabilitation Facilities; and
- Schools and Universities.
Testimonials
Judy Rosser, Blair Drug and Alcohol Program's Executive Director
Pennsylvania Single County Authority
“SBIRT has been vital in expanding the capacity to address substance use disorders in our communities. SBIRT has provided the framework to engage the physical health community in a meaningful way. SBIRT provides the tools needed to engage physical health providers in their identification of substance use/dependence, but also the skills to intervene early on a significant health issue. Integrating this work into the physical health system promotes better health outcomes overall.”
Dr. Zane Gates, MD, Co-founder of EMPOWER3 Center for Health
Primary Care Office
“The SBIRT program at our practice has enabled us to screen patients who otherwise would not have been screened, and has allowed patients to access services they otherwise would have not had access to. Providing SBIRT services has been an eye-opening experience for both practitioners and patients.”
Vince Capone, PA-C of EMPOWER3 Center for Health
Primary Care Office
“Utilizing SBIRT in our practice has created a sustainable and organized approach to engage our patients about drugs and alcohol. By engaging every patient, at every visit a dialogue and rapport have been developed with many patients that may have otherwise been eschewed and allowed issues around drug and alcohol to be viewed in context of the whole patient. Primary care is one of the frontlines in the otherwise asymmetric landscape of the opioid crisis, creating a method to engage patients in an empirically effective way has been invaluable.”
Tracy Bornick, Central Intake Coordinator at Mercer County Behavioral Health Commission
Pennsylvania Single County Authority
“We are pleased about the SBIRT project in our county and the accomplishments thus far. It is my hope that substance abuse screenings can be implemented in every single primary care office, not only in Mercer County and Pennsylvania, but Nation-wide…”
Student, UPMC Western Psychiatric Hospital
“In the outpatient psychiatry setting, you don’t have the luxury of hours with a patient. SBIRT (Screening, Brief Intervention, and Referral to Treatment) is an approach which allows you to maximize 10-15 minutes in understanding a patient’s context and eliciting change talk. Recently, I was working in an outpatient clinic and I had a young woman come in to talk about alcohol use. She had been using naltrexone and felt this was no longer working for her. As we began, I used open-ended questions to learn more about her story. She had struggled with an eating disorder as well as intimate partner violence, and she finally felt she was now in a healthy relationship. Using motivational interviewing (MI) techniques was incredibly important in demonstrating that I was truly listening, and it allowed her to guide the conversation. She started to become tearful and verbally stated “thank you for listening.” In using the MI techniques I was able to build rapport and learn my patient’s story within a few minutes, and she felt understood. Using reflection statements and patient-centered language was central to this. We then began moving towards Brief Intervention- using the same “how” and “what” questions, as well as reflections, I learned that attending AA meetings has worked for her in the past, but she had lost touch with her sponsor. She stated, “I really should get a new sponsor, I want to go back to that kind of life. I know I can do it again.” She identified a strategy, explained that past experience made her confident in this strategy, and explained that fear and a lack of connection to a big organization had been holding her back. When asked how motivated she was to find a new sponsor (on a scale of 1-10 ) she told me she was a 7/10, because she did not want to be overconfident. I employed the next strategy and asked why she was a 7 and not a 5, she explained that her children are big motivators in her life an she wants to stop using alcohol so she can be a better mother. In a matter of 10 minutes we were able to get to a point where she was expressing significant change talk, as well as articulating her stressors, motivators for change, and strategies to do so. We came to the “referral to treatment” piece and she was in the office looking up specific organizations close to her. She decided to call AA as well as another organization more based in religion, as that was an important aspect of her life. She stated that her goal with both was to find a sponsor who fits her best. Using the SBIRT model allowed me to maximize the 15 minutes I had with her, and it was our first time meeting each other."
Peter Kreckel, Pharmacist at Thompson Pharmacy
"As a community pharmacist I've been in the business of helping patients since 1981. Recently I completed my SBIRT training and have implemented the screening process in my store. Thanks to my student pharmacists, we have screened numerous patients using the screening tool provided by SBIRT. I had a patient who has been struggling with benzodiazepine use for a while. She has failed to be titrated off her current benzodiazapine, and asked me for help in withdrawing from this medication. Thanks to my SBIRT training I immediately provided her with the phone number for Blair Drug and Alcohol Prevention. They provided my patient with the name of a local facility, where she will get the help she needs. Although she was not screened through the SBIRT process, the knowledge gained from the training allowed me to refer her for appropriate treatment. The most important thing I've learned from this training, is that our patients are not simply pharmacokinetic equations. They are real people with real needs that can sometimes can only be met outside the four walls of the pharmacy."